
Trust is foundational to health care. When patients perceive medical settings as unsafe or risky, avoidance of care becomes a natural, rational response with measurable clinical consequences. In a recent correspondence in The New England Journal of Medicine, titled “We Do Care,” Bernard E. Trappey, MD, writing on behalf of Minnesota Physician Voices, describes how fear related to immigration enforcement has led patients to delay or forgo medical care, resulting in preventable morbidity and adverse outcomes.1 Although the letter focuses on frontline clinical experiences, its implications extend well beyond the immediate encounter. For the blood community, particularly those engaged in maternal–child health and cord blood banking, fear-driven care avoidance raises a critical and underrecognized ethical challenge.
Reminders:
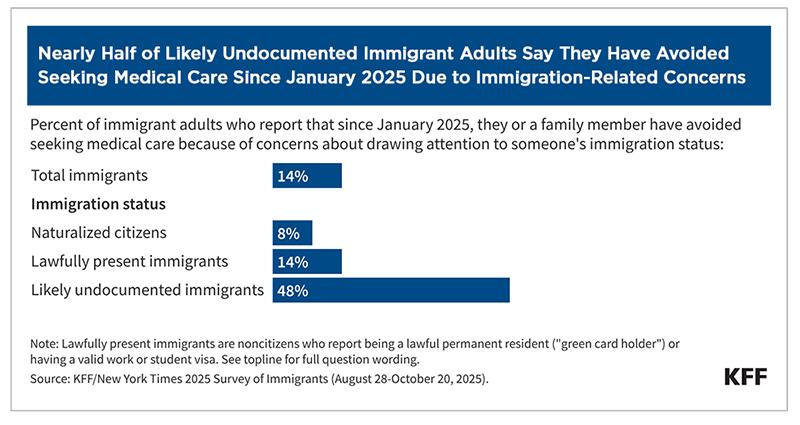
The mechanism described in Trappey and his colleagues is supported by substantial public health literature. Enforcement-related fear and hostile policy environments are associated with reduced health care utilization among immigrant and mixed-status families, including preventive and maternal services.
From an ethics perspective, fear operates as a structural determinant of health. It is a predictable response to external conditions. When such conditions disproportionately affect specific populations, they create population-level harms that challenge the principles of nonmaleficence and justice that underpin health care ethics.
Cord blood banking depends precisely on the elements that fear erodes. Prenatal visits enable education about cord blood donation and allow families time to consider informed consent. Prenatal testing and documentation are necessary to qualify units for banking and eventual release. Planned, hospital-based deliveries allow for sterile collection and an appropriate chain of custody.
When fear disproportionately affects communities that already face barriers to health care access, the result is a less diverse cord blood inventory and reduced transplant options for patients from those same communities.
When pregnant individuals delay care or deliver outside structured health care systems, cord blood units are either not collected or must be discarded due to incomplete screening or documentation. These losses are permanent. Unlike adult blood donation, there is no second opportunity to collect cord blood from a given birth.
Importantly, these losses are not evenly distributed. Public cord blood inventories rely heavily on donations from racially and ethnically diverse populations to ensure adequate HLA representation for patients who often lack suitably matched adult donors. When fear disproportionately affects communities that already face barriers to health care access, the result is a less diverse cord blood inventory and reduced transplant options for patients from those same communities.
Cord blood banking introduces ethical considerations that extend beyond individual donors. Public cord blood units are collected and maintained as a shared resource for unknown future patients. Many of these patients are pediatric recipients and individuals from underrepresented genetic backgrounds, and they depend on cord blood precisely because matched adult donors are unavailable.
Under the principle of nonmaleficence, harm occurs when foreseeable conditions reduce access to life-saving therapies. Fear-driven avoidance of prenatal and delivery care predictably reduces the availability of qualified cord blood units. Justice is implicated when these losses disproportionately affect populations already facing inequities in transplant access. Beneficence is undermined when present-day barriers to care erode future clinical benefit, and stewardship is compromised when scarce, publicly purposed resources are systematically lost. Losses associated with avoidable structural barriers pose not only ethical concerns but also inefficiencies that undermine national transplant preparedness.
The ethical concern is not the intent of activities that may frighten patients away from health care facilities, but their secondary effects on health care engagement, maternal-child outcomes and transplant readiness. From a transfusion medicine perspective, any condition that predictably reduces access to care and weakens biobanking infrastructure deserves attention.
Organizations such as AABB, which emphasize patient safety, are well-positioned to recognize fear-driven care avoidance as a determinant of blood and biotherapies availability. Protecting access to prenatal care and reinforcing health care settings as trusted spaces align with core principles of transfusion ethics and national preparedness goals. Fear in times of immigration raids creates a climate that shapes transplant readiness.
Cord blood banking illustrates how present-day barriers to care can shape future therapeutic options. When prenatal engagement declines, the consequences are felt years later by patients searching for a transplant match. In this sense, fear-driven care avoidance represents an intergenerational ethics issue: decisions and conditions affecting today’s pregnant individuals influence tomorrow’s transplant outcomes.
Fear that discourages pregnant individuals from seeking care is not only a maternal-child health concern; it is a cord blood and biobanking ethics issue with direct implications for transplant equity and preparedness.
By Ludwig Frontier, MD, MSc, MBA, DHSc, Contributing Writer
February 2026
 View Issue
View Issue
BACK TO ISSUE
February 2026
Transfusion is AABB’s scholarly, peer-reviewed monthly journal, publishing the latest on technological advances, clinical research and controversial issues related to transfusion medicine, blood banking, biotherapies and tissue transplantation. Access of Transfusion is free to all AABB members.
Learn More About Transfusion Journal
Keep abreast of what's happening in the field of biotherapies with CellSource - AABB's monthly update on the latest biotherapies news.

To submit news about the blood and biotherapies field to AABB, please email news@aabb.org.






President
Jose Cancelas, MD, PhD, CABP
Chief Executive Officer
Debra Ben Avram, FASAE, CAE
Chief Communications and Engagement Officer
Julia Zimmerman
Director of Marketing and Communications
Jay Lewis, MPH
Managing Editor
Kendra Y. Mims, MFA
Senior Communications Manager
Drew Case
AABB News
(ISSN 1523939X) is published monthly, except for the combined November/December issue for the members of AABB; 4550 Montgomery Avenue; Suite 700 North Tower; Bethesda, MD 20814.
AABB is an international, not-for-profit association representing individuals and institutions involved in transfusion medicine, cellular therapies and patient blood management. The association is committed to improving health by developing and delivering standards, accreditation and educational programs that focus on optimizing patient and donor care and safety.
+1.301.907.6977
Email: news@aabb.org
Website: www.aabb.org
Copyright 2025 by AABB.
Views and opinions expressed in AABB News are not necessarily endorsed by AABB unless expressly stated.
Notice to Copiers: Reproduction in whole or part is strictly prohibited unless written permission has been granted by the publisher. AABB members need not obtain prior permission if proper credit is given.


4550 Montgomery Avenue
Suite 700, North Tower
Bethesda, MD 20814
301.907.6977